Is It Mental Illness or Spiritual Attack? How to Discern the Difference
For anyone experiencing profound psychological or emotional distress, the boundary between mental suffering and spiritual struggle can feel terrifyingly thin. When faced with deep depression, intrusive thoughts, or sudden behavioral shifts, a critical question arises: is this a spiritual attack or mental illness?
In our modern culture, two dangerous extremes dominate this conversation:
- Secular Reductionism: The belief that all spiritual experiences, trials, and struggles are merely misfiring neurotransmitters or clinical psychiatric disorders.
- Hyper-Spiritualization: The belief that every mental health struggle, from clinical depression to bipolar disorder, is the direct result of demonic oppression or lack of faith.
Both extremes cause immense harm. Misdiagnosing a medical condition as a spiritual affliction deprives a suffering person of life-saving psychiatric care. Conversely, dismissing a genuine spiritual trial as purely psychological ignores the root of a soul’s agony.
The Catholic Balance: Grace Builds Upon Nature
The Catholic Church avoids both pitfalls by holding a deeply balanced, intellectually rigorous view. This perspective is anchored in the foundational principle of St. Thomas Aquinas: grace does not destroy nature, but perfects it (gratia non tollit naturam, sed perficit).
Faith and science are not competitors; they are complementary pathways to truth. The brain and the soul coexist in a profound, mysterious unity.
Therefore, caring for a suffering person requires addressing both their natural psychology and their supernatural reality.
Quick Answer: How Does the Catholic Church Distinguish Between Spiritual Attack and Mental Illness?
Under Catholic protocol, the Church distinguishes a spiritual attack or mental illness through a process of strict differential discernment. This mandate requires ruling out all natural psychological, psychiatric, and medical causes first through professional clinical evaluations.
Only when natural causes fail to explain specific, extraordinary signs (such as a violent aversion to the sacred, unlearned languages, or hidden knowledge) does the Church proceed with extraordinary spiritual interventions like exorcism.
Table of Contents
The Medical Mandate: Why the Catholic Church Demands Science First
Popular culture often portrays Catholic exorcists as rogue figures rushing into dark rooms with holy water at the first sign of strange behavior. The reality is the exact opposite.
The Catholic Church operates under one of the most cautious, scientifically rigorous, and bureaucratic protocols in the world when investigating extraordinary spiritual phenomena.
The Canonical Protocol
Under Canon Law (specifically Canon 1172), no priest can perform a solemn exorcism without the express, written permission of the local bishop. To obtain this permission, diocesan protocols mandate a exhaustive preliminary investigation.
The primary governing document for these interventions is the Vatican’s revised rite of exorcism, De Exorcismis et Supplicationibus Quibusdam (Of Exorcisms and Certain Supplications). This text explicitly dictates that an exorcist must not proceed to the rite of exorcism unless he has ruled out natural, physical, or psychological conditions.
To execute this mandate, dioceses form discernment teams that include:
- Licensed psychiatrists and clinical psychologists
- Medical doctors and neurologists
- Experienced spiritual directors and theologians
Before a priest ever recites a prayer of deliverance or exorcism, the individual under distress must undergo comprehensive medical and psychiatric evaluations. The goal is to establish a rigorous differential diagnosis—a systematic process of elimination that ensures no natural ailment is left untreated.
[ Individual in Severe Distress ]
│
▼
[ Initial Pastoral Care ]
│
▼
[ Comprehensive Medical & Psychiatric Exams ]
│
┌────────────┴────────────┐
▼ ▼
[ Natural Causes Found ] [ Natural Causes Ruled Out ]
│ │
▼ ▼
[ Ongoing Clinical Therapy ] [ Diocesan Discernment for Spiritual Care ]
Why Demanding Science First is an Act of Faith
Skeptics might wonder why a Church believing in the supernatural would place so much emphasis on modern medicine. The answer lies in the Catholic understanding of Creation.
Seeking medical science first is not a sign of weak faith. Rather, it is an act of deep respect for God’s natural order. God created the physical laws governing human anatomy, neurology, and biochemistry.
To ignore a biological brain malfunction and treat it exclusively as a spiritual curse is to dismiss the natural tools of healing—medicine, therapy, and clinical psychology—that God has allowed humanity to discover.
True pastoral care treats the whole human person: body, mind, and soul. If an individual is suffering from untreated neurological conditions like epilepsy, or psychiatric disorders such as schizophrenia, treating their condition purely with spiritual warfare is not only ineffective; it is spiritually and physically dangerous.
The Church prioritizes medical science first because truth cannot contradict truth. We must honor the natural before we can accurately discern the supernatural.
Overlapping Symptoms: Where the Lines Blur
Because human beings are an integrated unity of body and soul, a disturbance in one realm inevitably echoes in the other.
This integration creates what clinical psychologists and theologians call “the copycat effect”—a phenomenon where natural psychiatric conditions manifest symptoms that closely mimic extraordinary spiritual distress. To discern correctly, one must understand how these conditions diverge.
Schizophrenia and Psychosis vs. Diabolical Influence
Psychosis, whether triggered by schizophrenia, severe bipolar disorder, or substance abuse, fundamentally alters a person’s perception of reality.
- The Clinical Reality: Individuals experiencing psychosis often suffer from auditory and visual hallucinations. They may hear voices that are hostile, commanding, or mocking. Crucially, these hallucinations and delusions are chaotic, highly disorganized, and lack external, objective verification.
- The Spiritual Difference: In cases of genuine diabolical influence, the manifestations are ordered, highly intelligent, and objective. A person under spiritual attack does not simply “hear voices” in their mind; they exhibit extraordinary phenomena that cannot be explained by a neurological malfunction, such as speaking complex, unlearned languages or reacting violently to blessed objects that have been completely hidden from their sight.
Severe Depression vs. Spiritual Desolation
A profound loss of joy, energy, and hope can stem from a biochemical imbalance or a deep spiritual trial.
- The Clinical Reality (Depression): Clinical depression is characterized by anhedonia—the physical inability to experience pleasure in any aspect of life. It is accompanied by vegetative symptoms like chronic fatigue, sleep disturbances, and motor retardation. The struggle is systemic, affecting the patient’s physical ability to perform basic daily tasks.
- The Spiritual Difference (Spiritual Desolation): Spiritual desolation—or the “Dark Night of the Soul” described by St. John of the Cross—is not characterized by clinical apathy. The individual undergoing a spiritual trial retains their normal cognitive and physical capacities but experiences a profound dryness in prayer and a perceived absence of God. Rather than feeling indifferent to everything (clinical depression), the soul in desolation feels an active, painful longing for God’s presence.
Obsessive-Compulsive Disorder (OCD) vs. Scrupulosity and Obsession
Intrusive thoughts can paralyze a person, but their origin dictates the remedy.
- The Clinical Reality (OCD / Scrupulosity): OCD manifests as repetitive, unwanted thoughts (obsessions) followed by ritualistic behaviors (compulsions) designed to ease the resulting anxiety. In religious contexts, this becomes scrupulosity—a psychological condition where a person is consumed by an irrational, agonizing fear of having committed a mortal sin. They may confess the same minor faults repeatedly, unable to accept forgiveness.
- The Spiritual Difference (Diabolical Obsession): While clinical OCD arises from localized brain circuitry, diabolical obsession involves an external, sudden, and highly aggressive mental assault. The thoughts and temptations are violently forced upon the mind from the outside, often accompanied by external paranormal activity, sudden aversion to holy things, and physical markings (such as unexplained scratches or bruises) that clinical anxiety cannot produce.
Quick-Reference Comparison Table
| Condition / Struggle | Clinical Features (Natural Psychology) | Spiritual Indicators (Supernatural) | Primary Remedy |
|---|---|---|---|
| Psychosis / Hallucinations | Disorganized speech, incoherent voices, lack of objective external verification, baseline intellectual decline. | Organized hostile intelligence, xenoglossy (unlearned languages), telekinesis, knowledge of secrets. | Medical treatment, psychiatric medication, clinical therapy. |
| Depression / Apathy | General anhedonia (cannot enjoy food, hobbies), physical lethargy, lack of motivation across all areas of life. | Painful longing for God, dryness strictly in prayer, normal baseline physical functioning in daily tasks. | Medical evaluation, lifestyle changes, spiritual direction. |
| OCD / Scrupulosity | Cyclical anxiety, obsessive fear of sin, compulsive confession, inability to accept pastoral reassurance. | Sudden external mental assaults, violent aversion to the sacred, physical phenomena/markings, quieted by spiritual authority. | Cognitive Behavioral Therapy (CBT), ERP, obedient spiritual direction. |
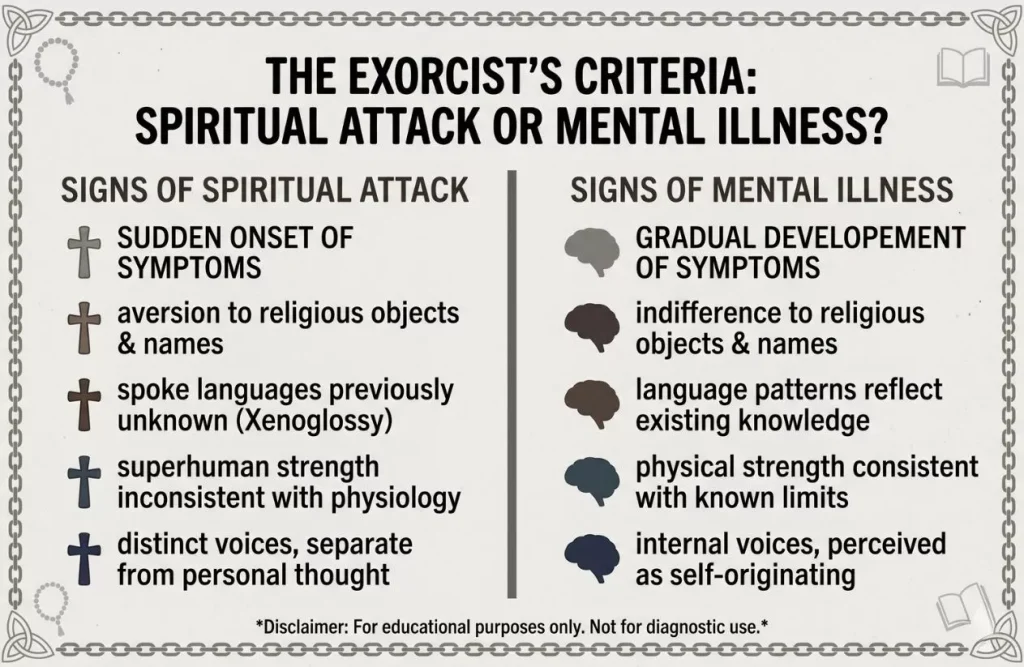
The Exorcist’s Criteria: The Strict Signs of the Extraordinary
When natural, medical, and psychological causes have been thoroughly investigated and ruled out by clinical professionals, the Church shifts its focus to spiritual discernment.
To determine whether an individual is experiencing extraordinary diabolical activity—such as possession or obsession—the priest-exorcist relies on precise criteria.
These criteria are not subjective impressions. They are ancient, objective diagnostic markers codified in the Rituale Romanum (Roman Ritual) of 1614 and meticulously preserved in the Vatican’s revised rite, De Exorcismis et Supplicationibus Quibusdam (Of Exorcisms and Certain Supplications).
An exorcist is strictly forbidden from declaring a case spiritual without the verified, sustained presence of these extraordinary signs.
The Four Classical Signs of Possession
Under Catholic protocol, a valid diagnosis of extraordinary spiritual affliction requires a convergence of specific, empirically observable phenomena. Isolated strange occurrences are insufficient. Exorcists look for the following four major indicators:
1. Xenoglossy (Speaking in Unlearned Tongues)
Xenoglossy is the ability to speak, read, write, or fully comprehend a language of which the individual has zero prior knowledge or natural exposure.
- The Clinical Reality: In high-stress psychiatric states, individuals may engage in glossolalia (unstructured, repetitive speaking in tongues or rhythmic babbling) or vocalize fragments of languages they heard in passing years prior.
- The Spiritual Indicator: True xenoglossy involves fluent, grammatically correct, and conversational command of complex, often ancient or dead languages (such as Latin, Biblical Greek, Aramaic, or regional dialects). The person can answer direct, unscripted questions in these languages, displaying an active intellectual comprehension rather than simple rote mimicry.
2. Occulta Cognitio (Revelation of Hidden Knowledge)
This sign involves the disclosure of distant, secret, or hidden facts that the afflicted person has no natural or technological way of knowing.
- The Clinical Reality: Highly perceptive individuals or those in heightened psychological states may pick up on subtle non-verbal cues (cold reading) to make accurate guesses about those around them.
- The Spiritual Indicator: Occulta cognitio transcends natural intuition. The individual may reveal deeply guarded personal secrets, unconfessed sins of the priest, private family details of a stranger in the room, or events occurring simultaneously miles away. This knowledge is shared with a hostile, targeted accuracy designed to intimidate or disrupt the discernment process.
3. Extraordinary Physical Strength
The display of physical power that completely defies the natural capacity of the individual’s age, health, and physical frame.
- The Clinical Reality: Adrenaline surges triggered by severe manic episodes, catatonic excitement, or acute psychosis can make a person incredibly difficult to restrain. However, this strength remains bound by the physical limits of human muscle mass and physiology.
- The Spiritual Indicator: Extraordinary strength in a spiritual context violates natural physical laws. A frail, bedridden elderly person or a young child might effortlessly throw multiple heavy, athletic men across a room, break high-tensile steel restraints, or manifest physical leverage that violates basic biomechanics.
4. Vehement Aversion to the Sacred
A violent, uncontrollable, and physical reaction to sacred objects, prayers, holy names, or sacramental rites.
- The Clinical Reality: An individual with psychological distress might exhibit emotional distress, anger, or theological opposition when confronted with religious symbols due to past trauma or intellectual dissent.
- The Spiritual Indicator: The reaction is involuntary, visceral, and frequently occurs when the sacred object is completely hidden from the individual’s physical senses. For example, the afflicted person might convulse, scream, or hiss when sprinkled with holy water that they were told was ordinary tap water, or react violently to a relic hidden inside a pocket, while remaining completely calm around ordinary, non-blessed equivalents.
The Dangerous Fallouts of Misdiagnosis
Failing to establish a rigorous boundary between a spiritual attack or mental illness carries grave pastoral, psychological, and physiological consequences. Misclassification in either direction damages the individual and distorts the healing ministry of the Church.
The Spiritual & Psychological Danger of Hyper-Spiritualization
When a clinical, neurological, or psychiatric condition is misdiagnosed as an extraordinary spiritual affliction, the results are often catastrophic.
- Clinical Regression: If someone suffering from clinical depression, bipolar disorder, or schizophrenia is advised to bypass psychiatric medicine in favor of deliverance prayer or exorcism, their underlying chemical imbalances go untreated. This neglect can lead to severe psychiatric decompensation, self-harm, or irreversible psychological deterioration.
- Iatrogenic Spiritual Trauma: When deliverance prayers fail to relieve clinical symptoms, the suffering individual is often told—or concludes on their own—that they lack sufficient faith, harbor hidden sin, or have been abandoned by God. This creates a devastating cycle of guilt, self-loathing, and spiritual despair, transforming a treatable medical condition into a severe crisis of faith.
The Danger of Secular Reductionism (Spiritual Neglect)
Conversely, assuming that all human distress begins and ends in the brain’s physical chemistry is equally destructive.
- Treating Symptoms while Ignoring Causes: When a genuine extraordinary spiritual oppression is treated solely with psychotropic medications, the physical symptoms may be numbed, but the underlying spiritual vulnerability remains wide open. The soul continues to experience deep, unaddressed agony because secular clinical therapy lacks the tools to engage supernatural realities.
- Pastoral Abandonment: Forcing a person undergoing spiritual trials to rely exclusively on secular psychiatry deprives them of the Church’s sacramental treasury. It leaves them isolated in a purely materialistic system that may treat their spiritual convictions as mere pathology, exacerbating their sense of isolation.
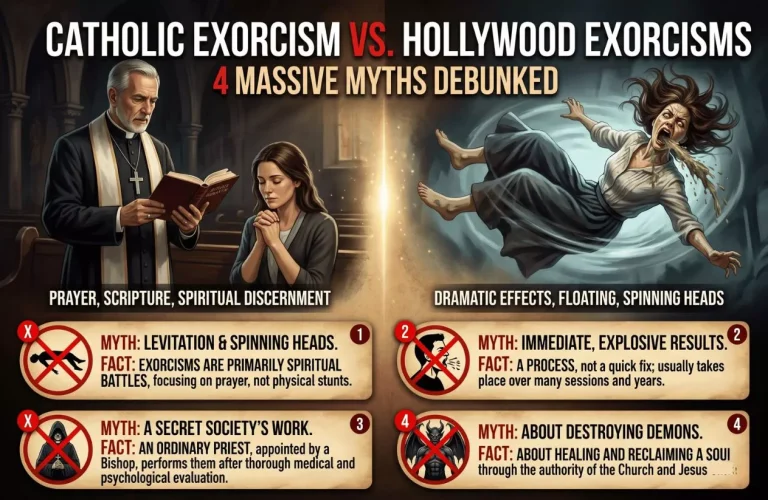
Related Article: Catholic Exorcism vs. Hollywood Exorcisms: Fascinating Myths Debunked
Practical Steps for Discernment: What to Do Next
When a person or their loved one is in the grip of terrifying distress, panic can make it tempting to search for extreme solutions. Discernment requires a calm, systematic, and grounded path.
To safely navigate deep psychological or spiritual trials, follow this structured, sequential framework.
Step 1: Secure a Comprehensive Medical and Psychiatric Evaluation
Before seeking spiritual interventions, rule out natural explanations. Schedule an appointment with a primary care physician and a licensed mental health professional.
- What to ask for: Request a full neurological screening, blood panels (to check thyroid levels, vitamin deficiencies, and toxicities), and a clinical psychological evaluation.
- Why this matters: Treating a chemical imbalance, a sleep disorder, or a neurological issue with spiritual warfare is highly ineffective and dangerous. Establishing a physical baseline first ensures that your biological health is fully cared for and protected.
Step 2: Establish a Stable, Sacramental Life
Do not seek extraordinary remedies before utilizing the ordinary means of grace. The Catholic Church teaches that the ordinary Sacraments are exponentially more powerful than any extraordinary rite of deliverance.
- The daily routine: Focus on the essentials. Attend Sunday Mass, go to Confession regularly, and spend quiet time in Eucharistic Adoration. Dedicate a short, consistent window each day to structured, liturgical prayers like the Rosary or the Liturgy of the Hours.
- Why this matters: A soul anchored in regular sacramental grace is highly protected. Consistent prayer grounds the mind, calms the nervous system, and provides the steady spiritual nourishment needed to endure any trial, whether natural or supernatural.
Step 3: Consult a Grounded Parish Priest
If distress persists despite medical care and a stable prayer life, schedule a pastoral meeting with your local parish priest.
- Who to avoid: Do not consult self-proclaimed “deliverance experts” on internet forums, anonymous social media groups, or unapproved spiritual ministries. These spaces often lack theological training and tend to foster paranoia, scrupulosity, and spiritual pride.
- Why this matters: A local diocesan priest is ordained, guided by canonical authority, and trained to provide balanced spiritual direction. He can assess the situation objectively, coordinate with local diocesan assessment teams, and help you navigate the process of obtaining formal spiritual assistance if extraordinary indicators are truly present.
Conclusion: Healing the Whole Person
True healing cannot occur in a vacuum that separates the body from the spirit. Humans are integrated creations, and the Catholic Church’s traditional approach to discernment respects this reality by refusing to compromise on either medical science or supernatural truth.
When navigating the complex, often terrifying terrain of a suspected spiritual attack or mental illness, we must reject the false choice between faith and reason. Seeking a psychiatric diagnosis, taking prescribed medication, or undergoing clinical counseling does not represent a deficit of faith. Instead, it respects the natural, biological order created by God.
At the same time, we must open our hearts to the supernatural support of the Sacraments, trust the quiet guidance of ordinary pastoral care, and find comfort in the truth that God heals the whole person. By integrating clinical accuracy with sacramental grace, we protect the vulnerable, honor the truth of Catholic tradition, and find a steady path out of darkness.
Related Article: The Saint Benedict Medal: The History and Meaning